Digital transformation strategy is no longer the sole domain of the CIO. Most savvy executives understand the transformational power of IT and they have really great insights on how to leverage IT. Does this mean that the role of the CIO is diminished? I think it means the role of the CIO is changing. Gone are the days where I spend time explaining IT concepts to executives. They have command of concepts such as the cloud, mobile and analytics. But understanding IT is different than delivering IT transformation. I believe the execution part of my job is increasingly important. While strategy is still important, organizations that execute with excellence will win.
In Retrospect, Meaningful Use transformed healthcare
This evening I was reflecting on how much healthcare IT has changed over my career. I became a CIO the 90s, when our medical records were still largely on paper. My fellow executives would ask me when we would have fully electronic records. My answer would always be that we were 5 years away. In fact that was my answer for 10 years.
I have to admit that the tipping point was the HITECH Act and Meaningful Use. I was critical of that program at the time. I argued that there wasn’t evidence that showed the program objectives were the things that best furthered the goals of the US healthcare system (improved quality and reduced cost). In retrospect, that didn’t matter. The flood of money that Meaningful Use brought to healthcare IT resulted in providers not only meeting the objectives, but making the changes necessary to finish the transition to fully electronic health records. Because of that, we have more actionable data at our finger tips. That data is used to better manage the care we provide and that patient experience.
The Skype Interview
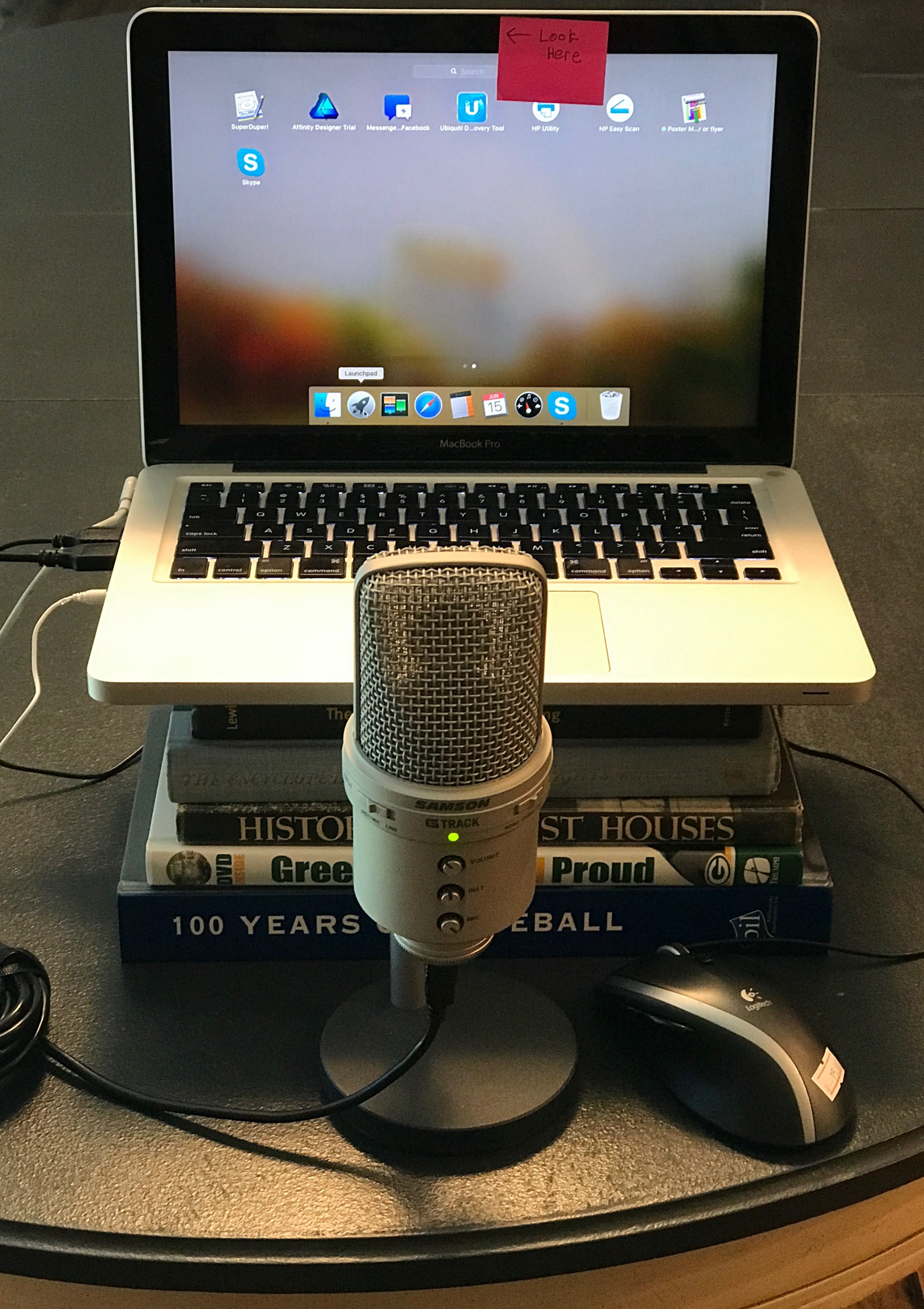
I have been thinking about other CIOs and IT pros looking for new gigs. I thought I would follow-up my last post with another learning from my recent search. Video calls are now a standard part of executive interviews. I want to share a few tips I think make for a good result.
- Place your camera at eye level. For me this means simply stacking some books under my Macbook. If you simply put a laptop on a tabletop you get the upshot angle, including a look into your nostrils. Be sure to frame your entire face and shoulders.
- Invest in a decent USB microphone. Laptop microphones are surprisingly good, but a high quality USB microphone (~$100) adds some clarity to your voice and that is the most important part of the interview.
- Your tendency is to look at the middle of the monitor to see the other party. And you should be looking at them for visual cues. But, you will also want to look squarely into the webcam to create the illusion of eye contact. As you can see in the photo of my setup, I put a sticky on the screen to remind me to look at the camera.
- Have an interesting, but not distracting, background. Even a plain wall with a plant to the side creates a more visually welcoming setting.
- Dress the part, at least the parts the interviewers can see.
Good luck!
Some thoughts about Customer Experience
I read a lot about digital transformation (especially in the twitter feed of @dchou117). It is an important topic. But, I believe it should be viewed as a means by which we achieve great customer experience. When we flex our digital transformation muscles without thinking through the ideal customer experience we end up with things like patient portals with single digit adoption rates.
Make no mistake, creating an ideal customer experience in any industry is difficult. It is especially difficult in large healthcare systems. Besides being incredibly complex, we have a legacy of applications, workflows and organizational culture that are significant barriers.
So, here is a suggestion for healthcare IT leaders…start with creating ideal customer experiences for your internal customers. Show your organization that IT has the vision and the chops to do this work and create a model for the external customer (patient) experience.
What is your organization’s customer experience when onboarding a new employee? Is it an all digital experience that is quick and well thought out? Does it collect only the minimal information required, without duplication? Are you using well designed front-ends and a database on the back end? Is it connected to the hiring process so nobody slips through the cracks or shows up to work without the ability to do their job?
What Employees Want
I think the best management advice I ever received was a reminder that I, as a leader, accomplish all of my work through the people on my team.
Therefore, my goals as a leader are:
- to make sure that the team members I am privileged to lead are happy, engaged, productive and
- those team members are working within a system of work that is continually optimized to accomplish clearly articulated goals quickly, cost-effectively and without defect.
That first leadership goal raises the question: What makes employees happy, engaged and productive? Over the years I have observed that most employees want the same things:
- Employees want to feel like they are part of a something important, a mission that transcends the daily activities of their workplace. Healthcare leaders are lucky because we have a great story to tell about caring for the people in our communities that is easily embraced. Lately I have expanded our mission to include transforming the healthcare system to provide better, safer and less expensive care.
- Employees want to feel that they bring meaningful contributions to the mission. Employees do not want to be over-managed. My greatest management mistakes were micro-managing employees. My greatest frustration as an employee was being micro-managed, especially when the supervisor was less capable. Leaders need to provide employees the big picture, direction, and periodic feedback – then get out of the way.
- Employees want to be recognized for their contributions. Studer Group provides great guidance to leaders on how to recognize employees.
- Employees want their leaders to have their backs, and in turn they will have yours. When the division as a whole lets down their customers the leader needs to accept responsibility, never singling out anybody in the organization. We are imperfect people. Mistakes are made. Leaders need to create a culture where we treat mistakes as learning opportunities and not times to dole out punishment. Leaders need to lead by example and admit when they make mistakes and to vow to learn from that mistake in order to do better in the future.
- Employees want leaders that ask them what they need to do their job better and what are management’s misconceptions that negatively impact productivity and quality. Employees can accept constraints if they understand them.
- Employees want to know managers are concerned about their satisfaction and continually gauging what can be done to improve the workplace, even if it is already a highly regarded workplace.
- Employees want to be surrounded by other high performers that have the same passion achievement and good work. That means leaders need to address performance issues in a timely and candid manner.
What would you add?
Eliminating the Interoperability Question
I just finished reading Victoria Brock’s excellent post Stop! Just stop with the “Interoperability”. In it she expresses the frustrations with healthcare systems vendors that represent their products as “interoperable” to non-IT buyers, knowing that those people will assume the best of what interoperability could mean. This is a phenomenon of human nature that I blogged about 12 years ago!
I agree with Brock. We need to educate our colleagues involved in reviewing clinical IT systems to stop asking the Interoperability Question. It is too vague and gives the vendors a chance to say yes to a different question than what is truly being asked. We need to train our non-IT colleagues to think about what they mean when they say interoperability. We need to give them examples of alternative questions, such as:
- How will the medication list in your system automatically reconcile with the medication list in our core EHR? Where have you done this?
- How will the allergy list in your system automatically reconcile with the medication list in our core EHR?
Brock reminds us that these interoperability questions involve three parties, the two application vendors and the client. Because something is possible doesn’t mean it will happen of all three parties are not committed to the work. We need to educate our colleagues that these interoperability questions cannot be answered by one party alone.
Those of us that are very clear about the the problem we are trying to solve and the new problems we are trying to avoid will have the most success.
Lyft and Blue Cross
Healthcare leaders should take note of this new partnership between Lyft and Blue Cross.
As a consumer, I like what Blue Cross is doing. While Blue Cross presents this as a way to improve access and reduce missed appointments, the next logical step is to quite literally steer patients to lowest cost providers.
There have been numerous studies that show the primary criteria patients use to choose their doctor and hospital is convenient location. Healthgrades summarized that finding in an infographic.
Perhaps the only thing more convenient than driving to the doctor’s office down the block is having a car waiting for you at your front door. The average cost of a Lyft ride is $12.53. It is a no-brainer for an insurer to pay $25 to steer a patient to a provider with a more favorable contract. Especially for expensive services such as chemotherapy or a Remicade infusion, both of which can run between $5,000 and $25,000 per visit.
Service Recovery After A Failure
In my inbox I received the communication from United Airlines about the changes they are making in response to their recent service failure. I thought it was well written, so I though this would be a good time to review one of my favorite topics. Every organization fails their customers at some point. Whether it be an unplanned EHR downtime, or dragging a paying customer off of a plane in a manner that upsets passengers.
Once the actual event has concluded there is a set of steps an organization should take to recover its standing with customers and to continually improve. These basic steps are the same for an IT team or an airline. In my opinion, United Airline’s initial response to recent events their response was terrible. Their subsequent efforts are on target. They followed the process that I have championed within my organization.
- Accept Full Responsibility: Accept full responsibility for not living up to your promise. Sure, the actions of others may have contributed to the incident. But, blaming others is deflection and not ownership. Ownership is empowering because it gives you the ability to fix the problem.I actually prefer to avoid apologies. I reserve apologies for personal failures and actions that are true negligence. Instead, I prefer to thank customers for their patience and their feedback and to let them know that we will work tirelessly to improve. A thank-you elevates a customer, it is a gift.
- Root Cause Analysis and Systemic Change: In United’s recent letter to customers they asked “How did this happen, and how can we do our best to ensure this never happens again?” Bingo. One needs to understand why it happened and make systemic changes to prevent recurrence. Root Cause Analysis (RCA) is a well understood science. Every CIO should understand RCA basics and they should have people on the team that are RCA experts. Finally, it is important to communicate to your internal customers the changes that you have made.
- Cultural Assessment: The extent to which the United CEO understands the cultural aspect of this situation is impressive. As the leader his language and the behavior will be reflected by the 87,000 United employees. While the team closest to the work should complete the root cause analysis, the leader must reflect with the leadership team regarding how organizational culture contributed to the event. Are financial constraints putting pressure on employees to move to quickly and skip steps? Is the lack of investment in employee development keeping people from meeting their full potential? Are leaders openly making negative comments about customers they should revere?
How does your organization handle service failures? What would you add to this approach?
The Importance of IT Customer Satisfaction Surveys
CIOs need to balance three goals:
- Advancing the organization’s strategy
- Engaging the IT team members
- Keeping customers happy
By customers, I mean the people that your IT organization provides services to. In my case it is doctors, nurses, and other knowledge workers. Some people call these people their “users”, but, as I have written in the past, that is a mistake.
Many IT Organizations Are Blind With Regard to Customer Satisfaction
I would argue these three goals are equally important. But, customer satisfaction is the most neglected. In my experience, most CIOs have all types of project portfolio reports that tell us how our strategic initiatives are doing. And, most organizations wisely survey their employees periodically to measure employee engagement and satisfaction. But, most CIOs do not have good overall metrics about customer satisfaction. Are you doing better than last year? Which IT provided services most need improvement according to your customers?
Sure, you might send help desk customers an after-call survey. But, that is a narrow measure of a single service. And quite frankly, these scores are largely meaningless. But, that is a blog post for another day.
Customer Satisfaction Is Important
An IT division can be completing all of their strategic projects with great success, and still be perceived within the organization as a failure if they are not meeting their customer’s expectations.
My Customer Satisfaction Story
I found (the hard way) that you really don’t know what your customers think of your service until you survey them in a methodical manner. I recommend all IT organizations survey their customers annually. In fact, all internal service providing organizations (HR, Legal, Finance, etc.) should join together to survey customers annually.
I thought the IT organization I led was providing good service until our first customer satisfaction survey: 71% of customers rated our service as good and great that year (ouch). My first reaction was to blame the customer and rationalize the data by claiming how difficult it is to provide good IT services. Once I got over that initial bout of self-pity I got to the business of identifying the area of greatest customer dissatisfaction (as surfaced by the survey and follow-up discussions). Our IT team developed a plan to improve those areas. Every year we would get more feedback and every year we would develop improvement plans.
In our last survey 92% of our customers ranked our service as good or excellent. This year-over-year improvement has been my most cherished accomplishment. It was also one of the greatest sources of motivation for the IT team members. They loved hearing the comments and seeing the scores.
Happy To Help
I am happy to share the survey tools that I have used. I am also happy to share my aggregated results if you want to benchmark your results.
Don’t Hijack Physician Workflow
During my time off I have been meeting with folks to see what is new in the healthcare IT space. I got a quick demo of a product called IllumiCare. Their mission is to provide cost information to physicians so they can make informed, cost-effective decisions about plans of care and hospital orders.
To be clear, this is not an IllumiCare endorsement and IllumiCare did not ask me to post this. I just saw a demo. But, their offering is based on 2 principles that I completely agree with. I believe these should be guiding principles for all of us in healthcare IT:
1. Embed everything in the EHR
Illumicare’s information is presented as embedded panes in EHRs such as Cerner or Epic. Illumicare believes (and I agree) that having separate systems kills adoption. Physicians live in the EHR. They don’t want to login to separate systems; re-query their patients; nor deal with different user interfaces. Even if you have single sign-on and patient context management, there is significant inertia that keeps physicians from logging into other systems.
2. Don’t hijack the physician workflow
Our attempts to build alerts into the physician online ordering workflow have been failures. Because these alerts are seldom relevant to the task at hand physicians clear these alerts before they are even observed. It is time to STOP using alerts except in the most critical safety situations.
Instead Illumicare presents cost information on review screens. The idea is that information is imparted when the physician is most open to receiving the information. Over time physicians come to understand the cost impacts of their behavior and modify that behavior over time.
